Community medicine
A rebel alliance of rare parents united as the PIGN-CDG Cure Collective to fund a drug repurposing project. One of the top 3 hits is ascorbyl palmitate aka fat-soluble vitamin C - and it's working!


In collaboration with



 / Twitter")

Disclaimer
The results of the PIGN-CDG drug repurposing project that we are sharing in the spirit of open science below are novel preclinical research findings and therefore they do not constitute the practice of medicine. Please consult a physician or clinical care team if considering off-label use of any approved drug or compassionate use of any experimental drug. The same caution applies to nutraceuticals, supplements and “generally recognized as safe” compounds.
The PIGN-CDG Cure Collective gelled two years ago under the leadership of a pioneer family from New Jersey. Susie Lam and Hiran Patel, two British ex-pats residing in the outskirts of New York City, were mobilized by their daughter Alice’s diagnosis. CDG CARE, the umbrella foundation representing the 190+ Congenital Disorders of Glycosylation and recent awardee of the prestigious Rare As One capacity-building grant from the Chan Zuckerberg Initiative, served as a fiscal sponsor for the PIGN-CDG community, enabling highly motivated families to rally for research.
Longtime readers of Cure Odysseys surely recognize the abbreviation CDG by now.

Seasoned by years in finance — one of their secret superpowers — Susie and Hiran efficiently organized a community-driven, “by us, for us” fundraising campaign focused on drug repurposing using yeast avatars. A tried-and-true playbook successfully deployed by Perlara in partnership with a dozen CDG communities. The most recent example is DHDDS.
As CDGs go, PIGN-CDG is more prevalent than some of the rarest subtypes, but still qualifies as ultra-rare. A one-in-a-million genetic lightning strike with the destructive force to forever alter a family, and at the same time, the generative spark for a cure collective. It shouldn’t be up to rare disease parents to make medicines for their sick kids. The harsh reality is that no one else is stepping up to the plate with dollars and devotion for rare genetic diseases that nobody has heard of except the people living with them, day in and day out.
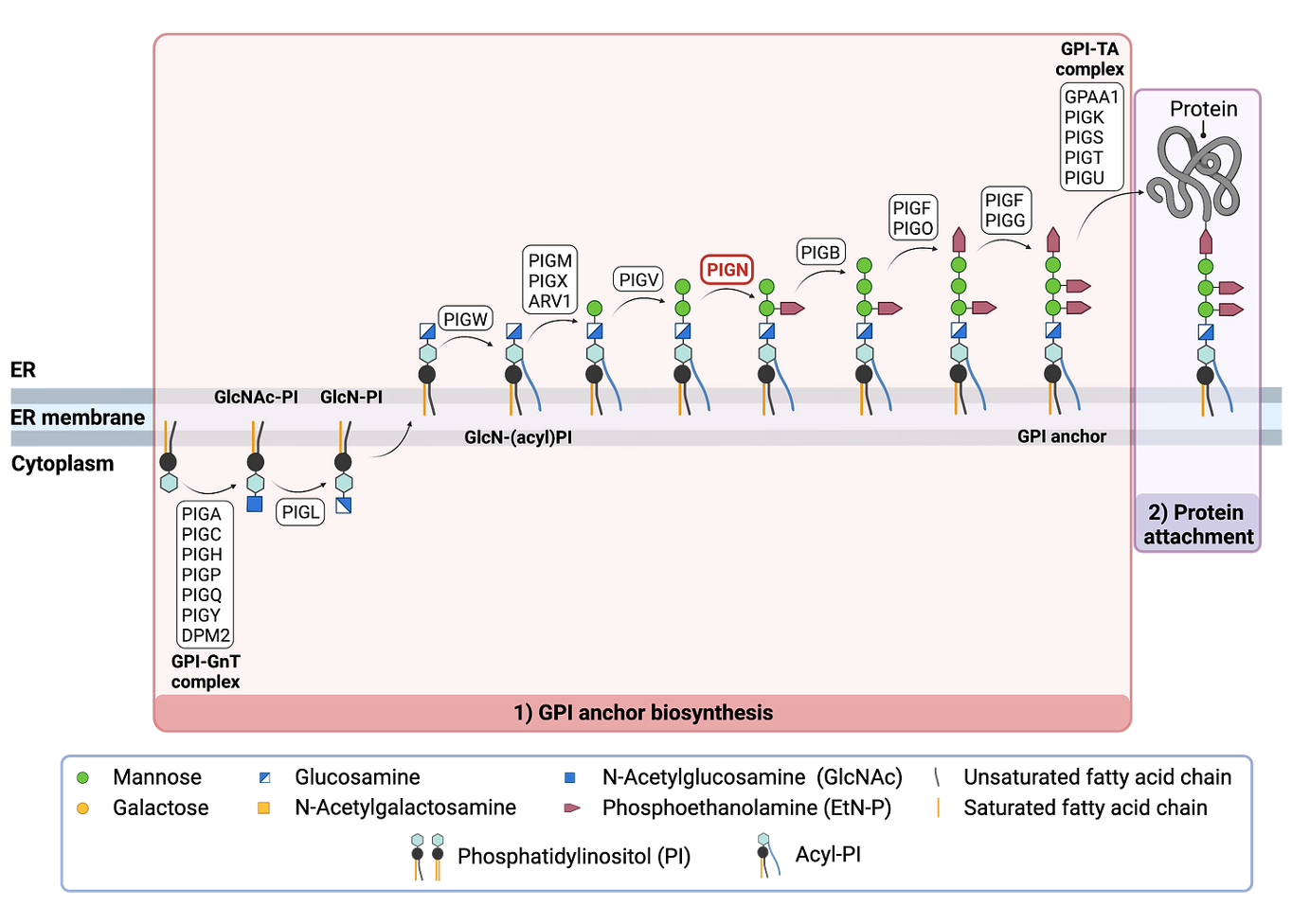
But first a quick glycosylation fresher. PIGN is one of 24 enzymes employed in a buzzing factory that assembles GPI anchors on both sides of the endoplasmic reticulum membrane. You can think of a GPI anchor as the foundation on top of which a prefab house, or in this case a protein, is mounted. The PIGN enzyme is located smack dab in the middle of the assembly line.
You can get caught up to speed on the last project update from a year ago. Right after we completed a test-flight screen of the ~2,000-compound Pharmakon library, a best-of compilation of approved generic drugs and over-the-counter supplements you can order online. Before we dig into the details, let’s take a moment to compare the results of the PIGN Pharmakon screen to five other Pharmakon screens of yeast avatars of inherited metabolic diseases, four of which are fellow CDGs: PIGA, PIGS, PGAP3 and ALG11.
The plot below shows that the average yeast growth spans two logs, meaning some yeast avatars are inherently sicker than others. The SURF1 haploid and diploid screens serve as controls. The average yeast growth of the SURF1 diploid is 2-fold higher than the haploid, as expected given that diploid yeast cells are twice the size of haploid yeast cells.

The three-way comparison between PIGS, PIGA and PIGN is informative. The PIGN and PIGS Pharmakon screen both yielded relatively few rescuers. The PIGS Pharmakon screen identified more sensitizers than the PIGN Pharmakon screen. Overall, there are relatively few rescuers and sensitizers for PIGN. The PIGN yeast avatar is the sickest of the six yeast avatars we screened against the Pharmakon library.
Across the five CDG Pharmakon screens, there are relatively few rescuers compared to the SURF1 Pharmakon screens, indicating that it’s not the severity of the growth defect per se that results in fewer rescuers. The PGAP3 Pharmakon screen is an exception because the growth defect of the PGAP3 yeast avatar is leaky.
Why is the ability to rescue the PIGN yeast avatar low? It could mean that there are no robust compensatory mechanisms available to overcome a state of PIGN deficiency. Or the compensatory mechanisms just have a low ceiling. PIGN appears to be an exception among the five CDGs screened in terms of vulnerability to sensitizers, where PIGA takes the cake with ALG11 in hot pursuit, followed by PIGS. Interestingly, PIGN deficiency is difficult to rescue in yeast but at the same time also difficult to make worse.
Now let’s turn our attention to the PIGN Pharmakon screen results. Remarkably, a clear pharmacological class emerged as the winner of the PIGN Pharmakon screen. Half of the top 20 hits are azole antifungals, including the top four rescuers. Where did we see this same rescuer pattern before? Look no further than PIGS, the last stop on the GPI anchor biosynthesis assembly line.

A direct comparison between the PIGN Pharmakon screen and the PIGS Pharmakon screen shows that the PIGN and PIGS yeast avatars behave similarly, i.e,. they share a large fraction of rescuers and sensitizers. Does that mean perturbations to the second half of the GPI anchor biosynthesis pathway — the stops between PIGN and PIGS — result in a shared pathophysiological cascade that is somehow alleviated by a common rescue mechanism?

Notably, the atypical antipsychotic ziprasidone rescues the PIGN yeast avatar but not the PIGS yeast avatar. Antipsychotics are noteworthy in the context of drug repurposing for CDGs. Going back to Perlara’s first drug repurposing screen for a CDG, we found that aripiprazole was the top rescuer for NGLY1 deficiency. In the MAN1B1-CDG fly screen performed in collaboration with Prof Clement Chow’s lab at the University of Utah, and in the SRD5A3-CDG worm screen, we also saw antipsychotics come up as hits. Curiously, each CDG prefers its own antipsychotic for reasons that remain a polypharmacological mystery.
As luck would have it, we noticed the most clinically actionable hit shared between PIGN and PIGS is an over-the-counter supplement: ascorbyl palmitate, otherwise known by its street name: fat-soluble vitamin C. Ascorbyl palmitate turned out to be the star of the show, but we’ll get to that in a few moments.
Next we compared the PIGN Pharmakon screen to the PIGA Pharmakon screen. PIGA is an interesting comparison because it is the bookend to PIGS, kicking off the GPI anchor biosynthesis assembly line. We don’t see any common rescuers in either direction, except maybe, you guessed it, ascorbyl palmitate (albeit a very weak PIGA rescuer). None of the azoles were common rescuers; in fact a handful of azoles are PIGA sensitizers! The PIGN-selective rescuer ziprasidone does nothing for the PIGA yeast avatar.

The Pharmakon screening campaign taught us that the ability to compare different GPI anchor deficiencies reveals common disease modifying pathways and potential “platform in a pill” drugs, i.e., one medicine that treat a bundle of related rare genetic diseases.
At the outset of the project, we’d planned to screen the 8,400-compound TargetMol library after a successful Pharmakon pilot screen. Rewind the clock to the summer of 2023, when we generated the results summarized below.
The 8,400 TargetMol library compounds are distributed across 27 384-well plates. The Z score distributions for each of the 27 plates are individually displayed. The positive control (magenta points) is a wildtype (healthy) yeast strain. The negative control (cyan points) is the PIGN yeast avatar treated with placebo (compound-free solvent). Each of the orange points is a compound from the TargetMol library.
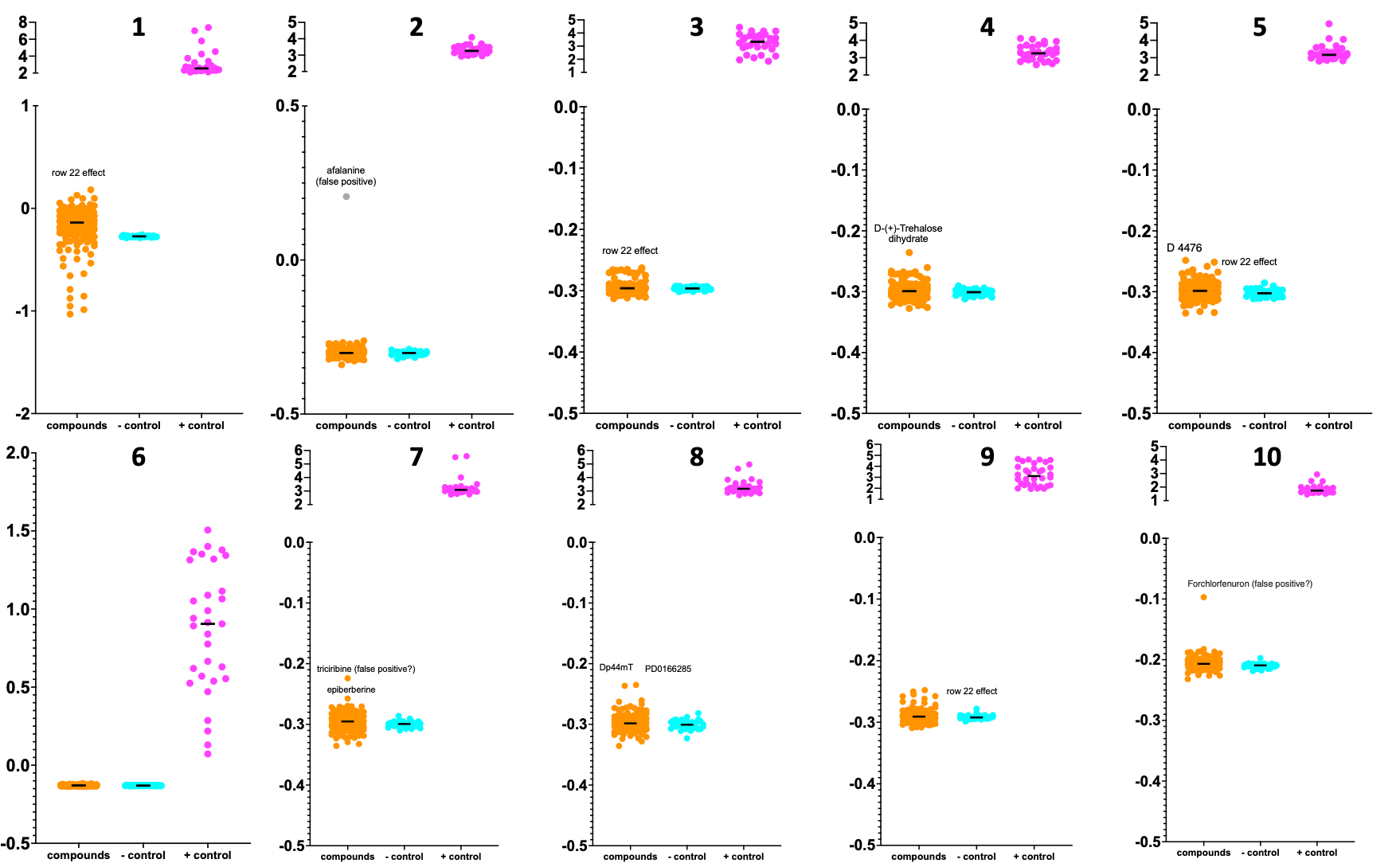
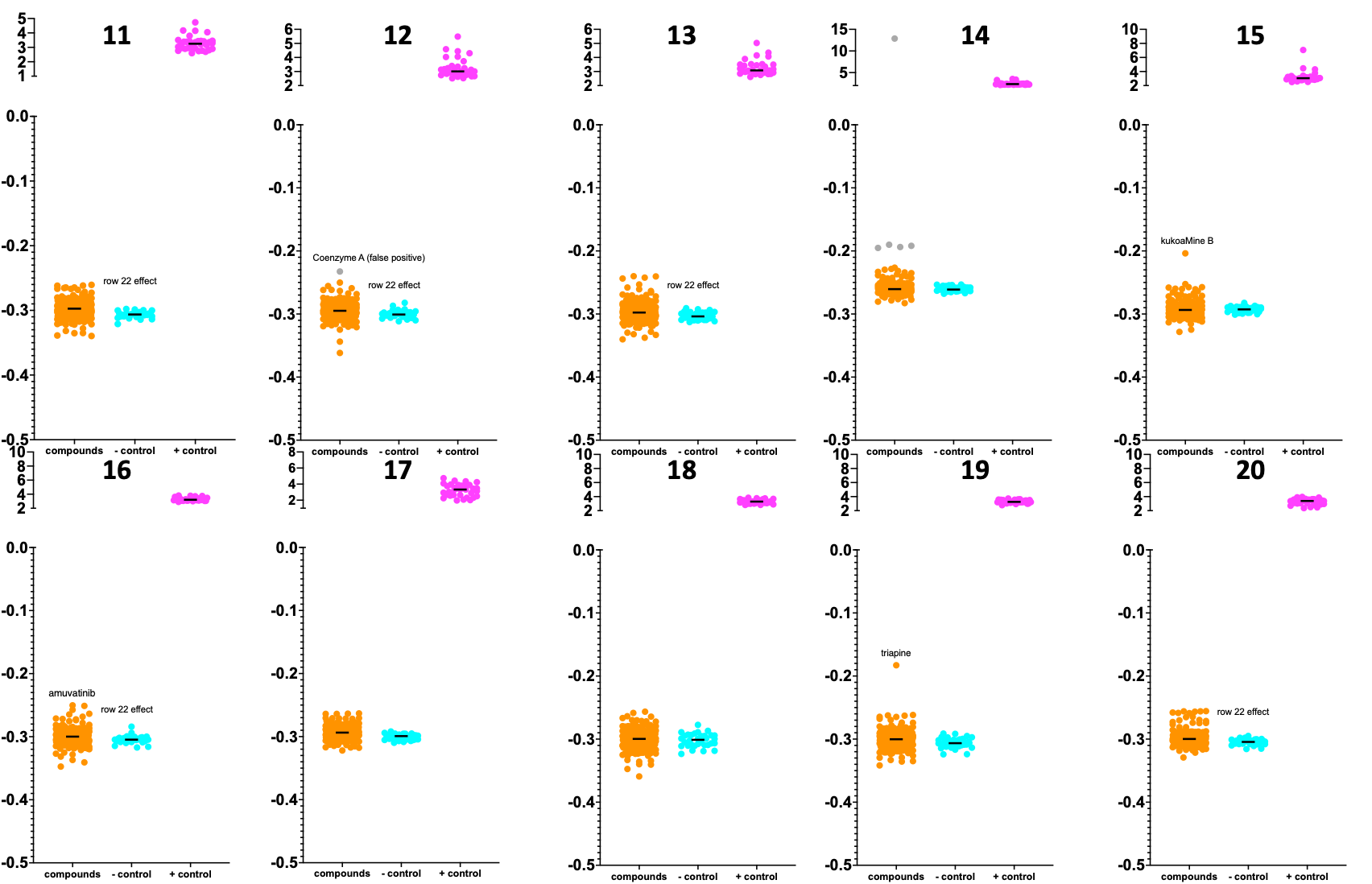

The PIGN TargetMol rescuers are weak to moderate, as we saw in the Pharmakon screen. The dearth of sensitizers was also observed in the expanded TargetMol screen. 13 rescuers from the combined TargetMol and Pharmakon screening campaigns were evaluated in dose-response validation experiments a year ago. Three finalists entered the winner’s circle.
In first place is voriconazole (posaconazole showed similar results). The azoles are the top pharmacological class overall and, reassuringly, the top hit from the Pharmakon screen is an azole. At the top dose tested at the 48-hour time point, voriconazole increased yeast growth by a whopping 300%. Voriconazole is approved for pediatric use but requires a prescription for off-label use.

So far everything checks out. In second place is ziprasidone. The kinetics of rescue by ziprasidone are slower than the kinetics of rescue by voriconazole. Could that mean ziprasidone targets a different mechanism of action, or acts further downstream? At the top dose tested at the 48-hour time point, ziprasidone increased yeast growth by 50%. Not too shabby. Ziprasidone (the brand name is Geodon) is also approved for use in children as young as 10 years old.

The third-place finisher is ascorbyl palmitate. Some of you reading this may already be taking ascorbyl palmitate as part of a daily supplement stack. The maximal growth rescue achieved by ascorbyl palmitate is 25%. Doesn’t seem that impressive, especially compared to the magnitude of rescue by voriconazole. But that could be due the stability and bioavailability of ascorbyl palmitate versus voriconazole in yeast media. Or differences in drug uptake into yeast cells among several other possibilities.

We don’t know how the therapeutic effect size in yeast correlates to the therapeutic effect size in humans. There’s really only one way to find out. So the PIGN-CDG Cure Collective advanced ascorbyl palmitate to what we call a 1-to-N trial, with Alice as the first PIGN-CDG ascorbyl palmitate pioneer. Ten other PIGN-CDG kiddos have followed her since.
In parallel, we are testing the top three PIGN yeast hits for rescue of GPI protein expression in PIGN-CDG patient fibroblasts. The PIGN-CDG Cure Collective organized fibroblast collections in the first phase of the project, so we have fibroblasts for almost every PIGN-CDG kiddo, including the ones who are taking ascorbyl palmitate as we speak, some of them for over a year now. I won’t keep you in suspense any longer.
In consultation with Dr Andrew Edmondson at CHOP, Alice began her N-of-1 trial 14 months ago. IRB and IND approvals are not necessary since anyone with an internet connection and $40 can order ascorbyl palmitate online. What about all the other variables? Bryan Johnson, arguably the N-of-1 messiah, receives the same legitimate criticism.
Parents have their kids on multi-component cocktails, not to mention physical and occupational therapy. Can we really assign therapeutic efficacy to a single intervention? Kids naturally have growth spurts even in a neurodevelopmental disease. How do we know that the ascorbyl palmitate is responsible for the benefits that are described below?

It’s not the job of a 1-to-N trial to answer those questions. The main purpose is to see if parents, the best and most sensitive detectors of change in their children, the humans who know them best, notice any changes one way or another. Ideally a validated clinical outcome measure already exists that objectively captures those changes. Another purpose is dose finding, since the optimal therapeutic dose will likely not be the same for all kiddos, especially for a naturally occurring essential metabolite like vitamin C.
There are two easy ways to mitigate parental bias. First, a group of pioneer patients should synchronize the intervention. Starting with a larger N allows for an estimation of the treatment response rate. We learned from the epalrestat PMM2-CDG experience not to over-index (or for that matter under-index) expectations based on the first pioneer patient’s experience. Second, keep everyone except the core caretakers — ideally just the parents — blinded about the n-of-1 trial. If a physical therapist or teacher who sees the child regularly corroborate what the parents are seeing at home, then the changes are not just wishful thinking.
On top of that we can add quantitative hard measurements. Seizures are common in PIGN-CDG. We didn’t know if seizures or ability to walk would respond to ascorbyl palmitate. Turns out they do!
Here’s a PIGN-CDG pioneer kiddo whom we’ll refer to as Patient 20. This is a before video, which shows that she is unable to take independent steps without active support and physical scaffolding.
Here’s Patient 20 after 9 months on ascorbyl palmitate. The video speaks for itself.
Some call it parental bias. I call it parental insights. Here are PIGN-CDG Cure Collective parents in their owns words describing the improvements they observed in their kiddos while on ascorbyl palmitate — and where available before vs after video capture evidence.
Patient 9:
I have been giving AP to my son for about 5, 6 months. Before starting I stopped all the supplements he was taking, waited about a month for him to clear everything, and did the lab research they recommended on the Drug repurposing project. Vitamin C levels were below normal when I started giving him AP. He was pretty worn out after a month without any supplements. At first it didn't seem to make any difference with or without AP, but I kept giving it. He began to recover after more than a month of taking 500 mg daily. So far, I have only been giving AP at the same dose, and after repeating the tests, the vitamin C levels had gone up. His behavior also changes, his body becomes more stable, he wants to walk and is constantly trying. He started to stand up on the furniture, he understands more, he doesn't get sick often (at least not once during the summer). I can't be sure that this is all due to AP, but I am sharing personal observations. We will be doing new lab research soon.
Patient 11:
Ever since we started ascorbyl palmitate, she didn’t have any seizures. So far, she is on keto and Lamotrigin, but it seemed like something changed a lot. She had an EEG and it looked a lot better than before. It really helps her, not in behavior matters or in changing her moods, but we still think that having no seizures is the greatest thing of all. The doctor said we have to wait a year before we can wean her off the medication or the ketogenic diet. It’s been more than half a year since her last big seizure.
Patient 17:
In our opinion he has made a lot of progress....certainly partly due to the ascorbyl palmitate and partly to a growth spurt, but in our opinion the association of progress is partly due to the vitamin. A before video:
He understands better, if we ask him simple things he understands more quickly, he copies our gestures a lot, he seems to have more muscle strength. Thursday 10 days ago he took his first 2 steps alone and now he walks short distances just giving him one hand. He has started to make some more noises like mamamamama papapapa which I hope will develop into dad and mum soon, or so it seems.
He points much more precisely, he recognizes us in photos and if you ask him where mummy is he points to me. He has added to the yes and no that he used to do with his head, the enough with sign language. Even with occupational therapy he seems better at movements and more precise. If someone shows him a movement he tries to copy, hit a ladle on the pot, build with duplo lego, use a screwdriver. An after video:
When I take him to sleep he does bye bye with hand to say goodnight. He has more sense of attachment towards me, if I wake up in the morning he cries because I go away (to the bathroom). From February to June he ate very little, he had lost weight. Since he took the vitamin his appetite returned and he regained the lost weight. Initially I thought it was related to the pancreas as per Alexa but luckily the enzyme is there, he only has a low pancreatic amylase value. Thinking about it now his appetite has improved a lot since he took ascorbyl palmitate, and in fact he has also added new foods that he didn't eat before like bread and pizza, pears and grapes, which he didn't even touch before.
The thing where he got worse is falling asleep, he has much more energy but he can't fall asleep and he never stays still for more than 5 minutes. Someone told me to give him the vitamin in the morning, since we give it in the morning he gets a little better in the evening but it happens that he is awake until 11pm and at 5am he already wants to get up, then cuddling him he falls asleep again for 1-2 hours. In the afternoon after lunch he is tired but only I can put him to sleep or sometime with other only in the stroller he collapses. He was already a light sleeper before and he struggled before but his hours of sleep have decreased.
Last year we had a polygraphy, he had a lot of sleep apnea.... in my opinion these have improved a little. Maybe it was because it was summer but the wheezing in the lungs has decreased and he also drools less (this could be because we lowered the depakine in May). He has become much more stubborn, if he gets his mind set on something he wants to do it, if he decides he wants to stand in front of the door he throws himself down making himself almost heavy so that we can't lift him and he has started to throw tantrums.
Recent update following an EEG:
No paroxysmal anomalies were observed as before, but he has not reached a stable sleep. For me it is the effect of the ascorbyl palmitate. The neurologist was impressed how he is much more active and cognitively alert. Now we too will remain for the next 6 months with unchanged drugs, in May we will decide whether to start reducing or removing the depakine. So in my opinion it is all related.
Patient 18:
Since starting it I’ve found that she recovers quicker after a seizure (she could eat dinner that night, usually she is in bed for 1 -2 days after seizures). She has had less illnesses (although this is compared to the flu season we went through a while ago). She has better appetite She has been making more sounds! (She is usually very quiet) and this a HUGE thing! Nowhere near talking but you get what I mean. Otherwise gross motor and fine motor is similar not much change. To be honest I don’t know if it’s coincidental or related to the medicine.
Community medicines are created by a community of personally affected families. Imagine a world where community governance and community ownership allows even the smallest rare disease communities to fund research, from concept to cure. That world is coming faster than you think thanks to the efforts and success of rare families like the PIGN-CDG Cure Collective. Onward!